Thoraxheelkunde. Topics uit de Thoraxheelkunde. prof em dr Toni Lerut, Definitie. Het is niet:heelkunde van hart en bloedvaten
|
|
|
- Ine Godelieve de Backer
- 5 jaren geleden
- Aantal bezoeken:
Transcriptie

1 Topics uit de Thoraxheelkunde prof em dr Toni Lerut, Emeritus Diensthoofd Thoraxheelkunde Universitaire Ziekenhuizen Leuven Thoraxheelkunde Definitie Het is niet:heelkunde van hart en bloedvaten 1
 Het is :heelkunde van het mediastinum 2")
2 Het is :heelkunde van het ademhalingsstelsel Trachea,Bronchi (windpipes),lungs Heelkundige aandoeningen Benigne: infecties v.b. tbc,aspergillosis Maligne: longkanker,long metastase v.b. colon,tracheale tumoren Long transplantatie voor end-stage respiratoire ziekten v.b.emphyseem,cystic fibrosis ( mucoviscidose) Het is :heelkunde van het mediastinum 2

 infectieus v.b.")
3 Het is:heelkunde van de pleura Heelkundige aandoeningen Mediastinum: tumoren v.b. thymoma, intrathorakale schildklier goiters Pleura: - Benigne:pneumothorax (klaplong) infectieus v.b.. abcess,empyema - Maligne :v.b. mesothelioma ( asbestos) maligne effusies Het is:heelkunde van de thoraxwand 3



4 Het is:heelkunde van het diaphragma Heelkundige aandoeningen Thoraxwand: Benigne:v.b.congenitale deformaties :pectus excavatum & carinatum v.b. infecties Maligne: thorax wand tumoren Diaphragma: Hernia,eventratie, Paralyse Trauma Het is :heelkunde van de slokdarm 4



5 Heelkundige aandoeningen Slokdarm: Benigne:v.b. reflux,hernia,achalasia,goedaardige tumoren,divertikels Maligne :kanker Thoraxheelkunde UZ Leuven Prof.Dr. Albert Lacquet 1932 eerste thoracale ingreep onder lachgas in België St Pieterhospitaal Leuven Rochester Minnesota Mayo De vaders van Thoracale Heelkunde in Leuven Campus St Barbara Pellenberg Campus St Raphaël 5

6 Universitaire Ziekenhuizen Leuven Dienst Thoraxheelkunde 1994 G.Deneffe D.Van Raemdonck T.Lerut P.De Leyn W.Coosemans Dienst Thoraxheelkunde 2018 Diensthoofd Prof.Dr. P. De Leyn Prof.Dr. H. Decaluwé Prof. Dr. P. Nafteux Prof. Dr. D. Van Raemdonck Prof. Dr. P. De Leyn Prof. Dr. W. Coosemans Dr. H. Van Veer Dr L.Depypere 6






7 Dienst Thoraxheelkunde 2018 Prof.Dr. H. Decaluwé Malignant & Benigne Lung tumors VATS Benign & inf ectious pleural disorders Pediatric pathology Prof. Dr. P. Nafteux Malignant & Benigne esophageal pathology Malignant pleural pathology Prof. Dr. D. Van Raemdonck LungTransplantation Lung Metastasis Mediastinal pathology Prof. Dr. P. De Leyn Malignant & Benigne Lung tumors Tracheal pathology Prof. Dr. W. Coosemans Functional esophageal pathology Chest wall pathology Diaphragm pathology Dr. H. Van Veer Chest wall pathology Esophageal pathology Dr Depypere Minimal inv asive surgery Esophagus and lung Totaal aantal ingrepen

8 Minimaal invasieve chirurgie /Keyhole surgery Longtransplantatie HL DL SL
9 9
10 Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus Incidentie - Epidemiologie 7000 nieuwe gevallen/jaar (België) mannen > vrouwen (3/1) Roken (Sigaretten) - 85% Mannen Prostaat : 30% Long : 17% Colorectaal : 13% Vrouwen Borst : 37% Colorectaal : 13% Long : 6% 10
 : 80% Spinocellulair")



11 5- jaars overleving Europa : 13% België : 15,4% Types Niet-kleincellig loncarcinoom (NSCLC) : 80% Spinocellulair carcinoom Adenocarcinoom Grootcellig ongedifferentieerd carcinoom Kleincellig longcarcinoom : 20% Zeer aggressief, snelle metastasering Behandeling vaak niet heelkundig Carcinoid tumor: 1 à 2% Goede prognose indien typisch carcinoïd en volledige resektie Klinische presentatie : twee vormen Centraal gelegen longcarcinoom o Typische symptomen Perifeer gelegen longcarcinoom o Zeer laattijdige symptomen 11
 -Retro-obstructieve pneumonie -Dyspnoe -Thoraxpijn (voorbeeld : pancoasttumor : perifere tumor) Nieuwe diagnose van longkanker *Oncologische evaluatie : zinvol?")
12 Symptomen op moment diagnose longkanker - 1/3 : Asymptomatisch (toevallige vondst) -1/3 : Symptomen van metastasen - 1/3 : Symptomatisch Algemene symptomen Thoracale symptomen -Hemoptoe -Prikkelhoest (veranderde hoest) -Retro-obstructieve pneumonie -Dyspnoe -Thoraxpijn (voorbeeld : pancoasttumor : perifere tumor) Nieuwe diagnose van longkanker *Oncologische evaluatie : zinvol? *Medische evaluatie : Kan patiënt ingreep aan? Slechts 20%-25% van patiënten met longkanker zijn potentieel uit curatief oogpunt behandelbaar (HK of RT) TNM Eight edition 12



13 T (Tumor) Gebaseerd op diameter tumor of ingroei T1 : tumor kleiner dan of gelijk aan 3 cm o o o T1a : 1cm T1b : > 1cm 2cm T1c : > 2cm 3cm T2 : Tumor groter dan 3 maar 5 cm o T2a : > 3cm 4cm o T2b : > 4cm 5cm T3 : o Tumor > 5 cm o Of aparte tumor nodules in zelfde kwab o Of ingroei wand, nervus frenicus, pericard o Of ingroei centrale longstructuren T4 o Tumor > 7 cm o Irresecabel : ingroei in organen vb hart, slokdarm T1c T



14 T3 Wandinvasie N (nodes) : locoregionale klieren N0 : geen klieren N1 : hilaire of interlobaire klieren N2 : ipsilaterale mediastinale klieren N3 : contralaterale mediastinale klieren Mediastinale klieren 14

")

15 Verdachte mediastinale klieren op CT en of PET : histologie of cytologie noodzakelijk Cervicale mediastinoscopie Punctie door luchtweg (EBUS-FNA) of door slokdarm (EUS-FNA) Invasieve stadiering van mediastinale klieren EBUS- TBFNA (via luchtweg) EUS-FNA (via slokdarm) Vrij betrouwbaar Minder complicaties dan mediastinoscopie Eerste keus (indien negatief, dan pas mediastinoscopie) EBUS EUS 15



16 Cervicale mediastinoscopie Lage morbiditeit Bijna geen contraindicaties Daghospitalisatie Ipsilaterale en contralaterale klieren Volledige mapping van mediastinale klieren Cervicale mediastinoscopie M (metastasen) M0 M1 o M1a : nodule in contralaterale o M1b : een enkele extrathoracale metastase o M1c : multiple extrathoracale metastases 16



17 T1aN0M1b TNM status Is gecorreleerd met overleving (op basis van internationale data verzameling) Is bepalend voor de behandeling 17
 behandeld worden Behandeling niet-kleincellig longcarcinoom Vroege")
18 Behandeling van niet-kleincellig longcarcinoom Hangt af van stadium van ziekte:oncologische operabiliteit o Vroeg stadium o Lokaal uitgebreide ziekte o Metastatische ziekte Hangt af van fitheid van patiënt:medische operabiliteit Slechts 20-25% van niet-kleincellige longtumoren kunnen radicaal (heelkundig of radiotherapeutisch) behandeld worden Behandeling niet-kleincellig longcarcinoom Vroege stadia T1-3N0-1 Heelkunde Bijkomende chemotherapie indien na de ingreep blijkt dat klieren aangetast zijn of diameter van tumor > 5 cm Tumoren < 4 cm : radicale radiotherapie (eventueel stereotactische radiotherapie) is valabel alternatief 18
19 Behandeling niet-kleincellig longcarcinoom Lokaal uitgebreide ziekte T4N0 of T1-3N2 Voorbehandeling met chemo of chemoradiotherapie (inductie therapie) Heelkunde bij respons Multi-level N2 pf N3 (contralaterale mediastinale klieren) : chemoradiotherapie Behandeling niet-kleincellig longcarcinoom Metastatische ziekte Chemotherapie Chemotherapie wordt meer en meer bepaald door type tumor : adenocarcinoom (Cis-Alimta) vs spinocellulair carcinoom (cis-gemcitabine) Moleculaire behandeling (voorbeeld tyrosine kinase inhibitoren indien Tumor EGFR positief) Immunotherapie Personalized therapy! Immunotherapie na chemoradiotherapie voor Stadium 3 tumoren (N2-N3) 19




20 Heelkundige behandeling - Anatomie - Wigexcisie - Pneumonectomie - Lobectomie-segmentectomie - Sleeve lobectomie - Thoraxwandresectie - Thoracoscopie VATS Sleeve lobectomie Longsparende procedure. Alternatief voor pneumonectomie Lobectomie + verwijderen van circulair deel van hoofdbronchus Bronchiale anastomose 20
")



21 THORAX SLEEVE LOBECTOMY FOR NSCLC Overall survival All patients (n = 77) 1 0,9 87,0 Survival Probability 0,8 0,7 0,6 0,5 0,4 0,3 67,5 57,0 48,8 45,6 0,2 0, Months Thoraxwand resectie Thoracoscopie of VATS : Video-assisted thoracoscopic surgery prof Van Raemdonck E0C93a




22 Thoracoscopie of VATS : Video-assisted thoracoscopic surgery VATS lobectomie (RATS) Chest 2013;143(5)(Suppl):e278S-e313S 22
23 UZ Leuven. cstage I cstage I VATS cstage I VATS converted to OPEN cstage I OPEN UZ Leuven. 120 cstage II-IV cstage II-IV VATS cstage II-IV VATS converted to OPEN cstage II-IV OPEN Postoperatief verloop na longresectie Mortaliteit Pneumonectomie : 6% Mortaliteit Lobectomie : 1 à 2% Duodenal switch : 1 % Gastric bypass : 0,5 % TKP : 0,3 % Electieve OPCAB : 0,2 % Lap Banding : 0,1 % Gemiddelde verblijfsduur : Pneumonectomie : 6 d Lobectomie : 7 d VATS Lobectomie : 4-5 d 23

24 Postoperatieve complicaties * Atelectase - mucus impactie - pneumonia * Arythmie (25%) * Broncho-pleurale fistel * Empyeem * Verlengd luchtlek Postpneumonectomie empyeem :levensbedreigend Etter in pneumonectomie holte Symptomen : koorts, malaise Diagnose : thoraxpunctie R/ Thoracoscopisch spoelen. Relook thoracotomies met wiekverbanden Eventueel thoraxvenster Resultaten : 5-jaars overleving Alle geopereerde patiënten ± 45% T1N % T3N0 ± 40% N1 ± 40% Chirurgie na inductie voor N2 ± 25% M+ 0% 24
=2500 pten/j - 1/3 : Symptomatisch Screening?")
=2500 pten/jaar - 1/3 : Symptomatisch Screening?")

25 Symptomen op moment diagose longkanker - 1/3 : Symptomen van metastasen - 1/3 : Asymptomatisch (toevallige vondst)=2500 pten/j - 1/3 : Symptomatisch Screening? Multidetector CT scan : sneden van 1 mm in one single breath (5 sec) lage radioactieve straling Hoge gevoeligheid om nodules te ontdekken Symptomen op moment diagose longkanker - 1/3 : Symptomen van metastasen - 1/3 : Asymptomatisch (toevallige vondst)=2500 pten/jaar - 1/3 : Symptomatisch Screening? Multidetector CT scan : sneden van 1 mm in one single breath (5 sec) lage radioactieve straling Hoge gevoeligheid om nodules te ontdekken computer aided diagnosis 3 maanden later Jeong et al., AJR 2007;18:
 Low dose CT N = 7915 Geen screening N = 7903 26")
26 National lung cancer screening trial National lung cancer screening trial 20 % reductie in Longkanker mortaliteit Nelson trial Nederlands - Leuven long screening onderzoek CT screening met baseline CT en nadien 3 CT s (na 1 jaar, na 2 jaar en na 2,5 jaar) Low dose CT N = 7915 Geen screening N =
27 IASLC TORONTO / Results Nelson Yousaf-Khan et al., in preparation Harry J. de Koning, Erasmus MC, Public Health Rotterdam Low dose CT control Diagnose long 148 x kanker Stadium I 70% x IASLC TORONTO / Results Nelson Lung cancer mortality rate ratio (95% CI) Year 8 Year 9 Year 10 MALES 0.75 P=0.015 ( ) 0.76 P=0.012 ( ) 0.74 P=0.003 ( ) FEMALES 0.39 P= ( ) 0.47 P= ( ) 0.61 P= ( ) Rand: FU: FU 94% complete year 10 Harry J. de Koning, Erasmus MC, Public Health Rotterdam Screening voor longkanker Gunstig effect. Studies in Europa voldoende matuur Heel wat nodules ontdekt. Strikt beleid noodzakelijk om nodeloze invasieve onderzoeken te ontdekken Gevaar overdiagnose Momenteel nog niet geïmplementeerd. Zeker jaarlijkse CT opvolging bij patiënten na heelkunde voor longkanker : second primary!!!! 27




28 Topics prof Van Raemdonck E0C93a longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus Pastorino U et al. J Thorac Cardiovasc Surg 1997;113:37-49 Long metastase solitair vs multipel peripheer vs centraal Scharp nodule 28


 - geen alternatieve betere therapie mogelijkheden vb.")
29 Long metastase Beeldvorming RX thorax CT PET prognostische indicatoren Volledigheid van resectie Aantal M+ 1 >< meerdere Ziektevrij interval Verdubbelingstijd M+ Histologie Kiemcel : best Melanoma : slechtst Mediastinale klieraantasting Indicaties voor resectie - volledige controle 1 tumor - perspectief op volledige resectie - afwezigheid extrathorakale M+ (~ colon - lever!) - geen alternatieve betere therapie mogelijkheden vb. chemo : kiemcel hormonaal : borst - voldoende fit 29





30 Wigexcisio Stapler Precisie excisie cautery - laser Cooper JD, Perelman M, et al. Ann Thorac Surg 1986;41:51-3 Toegang Thoracoscopie VATS Thoracotomie Sternotomie 30



31 UZ Leuven Prospective chirurgische database January 2002 December patients H Decaluwé 0 6.1% 21% 40.2% 17.3% 8.4% Resultaten 5YS 62.7% In-hospital mortality: 0% 90 day mortality: 0.5% 31
 n = 1907 1991-2018 ULB UCL ULg KUL UA n = 521 n = 315 n = 2 n = 1036 n = 34 UG n =")
32 Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus (H)LTx in Belgium Tx / center ( ) n = ULB UCL ULg KUL UA n = 521 n = 315 n = 2 n = 1036 n = 34 UG n = 1 32
 * Secundair (Eisenmenger s syndroom ~ CHD) (chronische longembolen CTEPH) Indicaties - respiratoir falen (zuurstof dependent) - levensverwachting < 12")
33 D Van Raemdonck G Verleden Terminale Longziekten PARENCHYM - Restrictief: bv longfibrose - Obstructief: bv emfyseem - Infectieus: bv mucoviscidose BLOEDVATEN - Pulmonale Arteriële Hypertensie (PAH) * Primair (idiopatisch, erfelijk, medicamenteus) * Secundair (Eisenmenger s syndroom ~ CHD) (chronische longembolen CTEPH) Indicaties - respiratoir falen (zuurstof dependent) - levensverwachting < 12 (tot 18) maanden - leeftijd < 65 y SL - < 60 y DL - < 50 y HL - ambulant - goede voedingstoestand - single orgaan falen - tolerantie voor immunosuppressieve medicatie - normale psycho-sociale status 33
 (LL) 1991-2017 N = 1036 90 80 70")

34 Types Hart-Long Tx (HL) Bilaterale Long Tx (BL) - sequential single (SSL) Unilaterale Long Tx - single Lobaire Long Tx (SL) (LL) N = HL DL SL N = /06/



35 (Heart)-Lung Tx in UZ Leuven per indicatie (n = 1036, 12/2017) ReTx 5% Eisenmenger 3% PH 5% Cystic Fibrosis 14% ILD 22% non-cf bronchiectasis 2% miscellaneous 2% alpha1 ATD 3% Emfyseem 45% Vos R, et al. Unpublished data N = HL DL SL Overleving SL >< BL 35
36 Overall survival UZ Leuven ( , n= 1036) 100 Overall survival, censored at redo-ltx Overall survival (%) years Time (years) n at risk n=230 Oldest LTx recipient alive now 80y! (SSLTx, emphysema, 2002) n=43 patients now >70 y old Wacht tijd (H-)LTx in UZ Leuven 8 months (vs. > 12mo. in ET) Deaths on waiting list 1% (vs. >10% in ET) Jaarverslag Raad voor Transplantatie UZ Leuven, 2016 Opting out wetgeving 36

37 Immunosuppressants 37



38 Statische Koude Preservatie Functionele Long in een doos 38
 Van Raemdonck et al.")

39 Commerciele Toestellen voor Ex Vivo Lung Perfusion (ELVP) Van Raemdonck et al. Transplant Int 2015; 28: Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus 39




40 Bulleus Emphysema Indicaties bullectomie - giant bulla met compressie onderliggend parenchym - verwikkeling bulla: - secundaire pneumothorax - infectie bulla - longkanker in bulla Bulleus Emphysema Dirk Van Raemdonck 40



41 VATS bullectomie Diffuus Emfyseem Patho-morphologie alveolaire destructie vergootte :alveoli & ductuli parenchymale destructie expiratoire luchtweg collaps 41



42 HYPERINFLATIE elastiche recoil van long verdwenen Dirk Van Raemdonck Remove dead space Relieve alveolar compression Improve elastic recoil Restore tethering effect Improve chest wall motion Improve diaphragmatic excursion Dirk Van Raemdonck 42

 - CO2 retentie: PCO2 > 50 mm Hg - Bridge naar Transplantatie - Oudere patienten bij wie")
43 Indicaties longvolumereductie - Hyperinflatie: RV > 250% - TLC > 125%; RV/TLC > Heterogeen emfyseem: bovenkwabben >> onderkwabben - Ernstig obstructief longlijden: ESW 20-30% - Diffusiecapaciteit: > 20% - Geen risicofactoren: - pulmonale hypertensie - te lage ESW DLCO < 20% ( vanishing lung ) - CO2 retentie: PCO2 > 50 mm Hg - Bridge naar Transplantatie - Oudere patienten bij wie transplantatie gecontraindiceerd is 43







44 De ideale patiënt Scintigraphie CT Bronchoscopisch : BLVR one way valve coil airway bypass Collaterale Ventilatie langs onvolledige fissuren! 44

45 LVRS UZ Leuven n = Dirk Van Raemdonck Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus Carter BW et al. J Thorac Oncol 2014;9: S97-S101 45
46 MEDIASTINALE TUMOREN - Thymus Tumoren - Lymphoma - Germ Cell Tumoren - Thyroid & Parathyroid tumoren - Neurogene Tumoren MEDIASTINALE TUMOREN Symptomen asymptomatisch algemeen locale paraneoplastisch ANTERIEUR MEDIASTINUM Incidentie 46




47 EPITHELIALE SUBTYPES Thymoma Thymus carcinoma Thymus carcinoid (NET) Differentiële Diagnose THYMOMA HYPERPLASIE Soms moeilijk Preoperatieve biopsie nodig? well encapsulated tumors NEEN Invasive tumors JA Cave droplet metastase 47










48 Mature Teratoma Cystic Teratoma Fat Sebum Bone Cartilage Bronchial epithelium Intestinal epithelium Pancreas Nerve tissue Thyroid Retrosternale Goiter Schwannoma VATS resectie 48




49 Bronchogene Cyste Mediastinoscopie VATS resectie Pericardiale Cyste «springwater cyst» Geen resectie VATS resectie enterogene cyste VATS resectie 49

50 Topics prof Van Raemdonck E0C93a longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarmkanker pectus SLOKDARMKANKER - Diagnose meestal in vergevorderd stadium ~ dysfagie wanneer 2/3 lumen vernauwd is 5- jaars overleving Europa : 13% België : 15,4% 50
 = meestal laattijdig Progressieve pijnloze dysfagie!")
51 Slokdarmkanker - Etiologie Roken en alcohol (vooral voor spinocell carcinoom) Barrett Adenocarcinoom o Risico x 50 o Screening! Incendentie neemt toe. Vooral adenocarcinoom distale 1/3 Symptomen: Obstructie dysfagie (2/3 stenose) = meestal laattijdig Progressieve pijnloze dysfagie!!! Anemie, bloeding Reflux gerelateerd Diagnose: Endoscopie met biopsie (F/U) met mogelijkheid tot eventueel behandeling (mucosale ca) Anatomische lokalisatie van de tumor Cervicaal Thoracaal bovenste 3 compartimenten middenste onderste. Cardia Distale 1/3 - GEJ : adenocarcinoom Proximale - mid 1/3 : spinocellulair epithelioma 51


 - Snel")

52 Barrett slokdarm Wit of parelmoer kleurig slijmvlies = plaveisel epitheel Barrett = abnormaal roze cilinderepitheel én dat intestinale metaplasie bevat Lijkt op maag slijmvlies dus diagnostiek op basis van microscopie en endoscopie Slokdarmkanker Diagnose meestal in een gevorderd stadium want: - Dysfagie : laattijdig symptoom (2/3 stenose) - Snel lympheklier aantasting Submucosale lymphatische plexus Lymfeklier aantasting: in 41-81% Tis 0 % T 1a 0-3 % T 1b % T % T % T % 52
 TNM slokdarmkanker Tis tot T4 : afhankelijk van penetratie diepte o Tis : Ca in")
53 Nieuwe diagnose van slokdarmkanker *Oncologische evaluatie : zinvol? *Medische evaluatie : Kan patiënt ingreep aan? Klinische staging: Endoscopie biopsie CT thorax - abdomen Echo endoscopie Bronchoscopie PET (PET/CT met correlatie) TNM slokdarmkanker Tis tot T4 : afhankelijk van penetratie diepte o Tis : Ca in situ o T1 : Tumor tot in lamina propria (T1a) of submucosa (T1b) o T2 : Uitbreiding tot in muscularis propria o T3 : Transmurale invasie o T4 : uitbreiding in mediastinale structuren 53
54 TNM slokdarmkanker N : o Nx : regionale klieren kunnen niet worden gevisualiseerd o N0 : geen regionale kliermetastasen o N1 : regionale lymphekliermetastase (1-2) o N2 : regionale lymfekliermetastase (3-6) o N3 : regionale lymfekliermetastase (>6) M : o Mx : Metastasen kunnen niet worden geëvalueerd o M0 : geen metastasen o M1 : metastase in verder gelegen klieren of organen Medische operabiliteit Longfunctie Cardiale investigatie Behandeling vroegtijdig stadium T1aN0M0 54



")



55 EMR EMR= zowel behandeling als staging T1a T1b + RFA EMR Beperkingen: o Verwikkelingen: Strictuur (circulair) Perforatie o Onvolledige ablatie / Verborgen klierbuizen o Soms meerdere sessies nodig o Cave: diepte van invasie T1b!! 55

56 Behandeling lokaal uitgebreid stadium ct1n+m0 ct2-4n+m0 Heelkunde indien locoregionaal geen invasie in omgevende organen geen metastasen. Inductie chemo-radiotherapie indie, grote tumor, klier aantasting, M+ klier in resecabel gebied. Palliatie Zo irresecabel, inoperabel of metastasen Inductie chemo-radiotherapy 56

57 Per type ypcr Adenoca: 23% Spino: 49% Heelkunde types: Slokdarmlichaam GEJ: Subtotale oesofagectomie, partiële gastrectomie, maagtubulatie en cervicale anastomose GEJ (> 5cm invasie maag) subcardia: Totale gastrectomie, Roux-en-Y jejunum VOORKEUREN TOEGANG Right thoracotomy, laparotomy, cervical anastomosis, gastric tube carina Left thoracoabdominal, cervical anastomosis, gastric tube cardia Left thoracoabdominal, thoracic anastomosis, gastrectomy + Roux en Y 57







58 En bloc resectie R0!! uitgebreide lymphadenectomie Minimaal Invasieve Esophagectomie ( MIE) LAPAROSCOPIE THORACOSCOPIE RECHTS (VATS) 58





59 INSTALLATIE Abdominaal Thoracaal RESULTATEN Chirurgische parameters: OE MIE p=0,01 p=0,001 Nafteux, Eur J Cardiothor Surg 2011 RESULTATEN Morbiditeit: OE MIE p=0,02 p=0,008 p=0,005 Nafteux, Eur J Cardiothor Surg



60 Role Functioning LEVENSKWALITEIT MIE OE Fatigue P=0,09 Pain general P=0, Role functioning p= PreOP PostOP PostOP PostOP PostOP 1-3 mo 4-6 mo 7-9 mo mo Nafteux, Eur J Cardiothor Surg 2011 Functionele resultaten-sequellen postoperatief - Volheidsgevoel - reservoirfunctie - Postvagotomie: - diarrhee - dumping - Anastomotische strictuur dilataties - Pylooroutlet obstructie dilatatie/botox - Reflux esophagitis Barrett PPI Na 1 jaar: 85% uitstekend zeer goed 1. FOTO 1.2. klinische activiteit 60
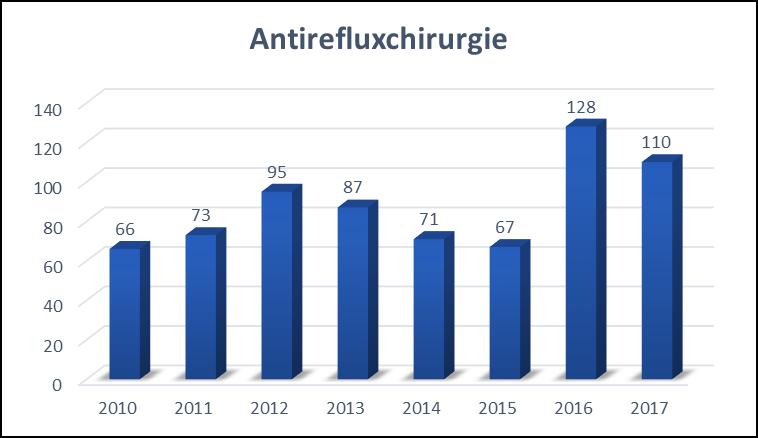
61 Slokdarmcarcinoom KCE Report 2012 Nood voor centralisatie! Enhanced Recovery Protocol (ERP) Enhanced Recovery Protocol (ERP) 61



62 Overleving na heelkunde Resultaten Oncologisch: heterogeen actueel: globaal 25-45% 5-jaar overleving - Leuven: 42% Stadium I 60-90% IIa 25-82% IIb 38-71% III 12-56% IV 0-31% Kwaliteit: Outcome ~ volume ervaring Palliatie: stents brachytherapie Zo irresecabel, inoperabel of metastasen Topics longkanker long metastasen longtransplantatie long volume reductie mediastinum slokdarm pectus prof Van Raemdonck E0C93a

63 Stoornissen van het sternum en thorax wand Pectus deformaties (excavatum, carinatum, arcuatum) Sternale fissuur Thorakale dystrophie (Jeune s disease) Poland s syndroom Tumoren van de ribben en sternum Pectus deformaties: oorzaak Dysfunctie van het diaphragma Abnormaliteiten in de rib morphogenese en groei Ongebalanceerde uitgroei van rib kraakbeen resulterend in verplaatsing van het sternum Pectus Carinatum Chicken breast, pigeon breast,kippenborst 63

 EKG")
64 Pectus excavatum Funnel Chest,Trechterborst Pectus excavatum: symptomen Pulmonaal: o intrathoracaal volume o respiratoire excursie tgv thoracale rigiditeit Cardiovasculair o Anterieure indentatie op rechter ventrikel o stroke volume and cardiale output Pectus deformititeiten: diagnose Inspectie Klinisch onderzoek RX Thorax CT-scan (Haller index) EKG Long functie testen 64

 Long functie")



65 Pectus : indicaties heelkunde Haller index > (PE) Long functie stoornis Cardiale compressie Progressie van de deformitiet Pijn thorax wand Self-image: functioneel well-being Open chirurgie :Ravitch Techniek 65







66 Pectus excavatum Minimaal invasief VATS :Nuss procedure Nuss, Journal of Pediatric Surgery, 33(4), , Pectus excavatum: Nuss 66








67 Pectus excavatum: Nuss Pectus excavatum: Nuss Pectus excavatum: Nuss 67


68 202 Resultaten Inspannings capaciteit A lot better Better No change Worse A lot worse 26,47% 38,24% 32,35% 0% 2,94% 64,71% Results Tevredenheid Extremely satisfied Very satisfied Satisfied Unsatisfied Very unsatisfied 1,18% 21,76% 51,76% 22,35% 2,94% 95,88% 68


")

69 Pectus Carinatum 2004 Presternal extrathoracic Reverse Nuss Abramson Journal of Pediatric Surgery, Volume 44, Issue 1, 2009, Thorax Heelkunde Brede waaier aan,dikwijls complexe,pathologiën Vooruitgang in beeldvorming heeft diagnostiek in hoge mate verbeterd Multidisciplinariteit = sleutel tot optimale indicatie stelling& therapie ( meer en meer gepersonaliseerd ) Sterke evolutie in ontwikkeling nieuwe heelkundige technieken en technologiën prof Van Hoog Raemdonck volume E0C93a =Expertise 207= optimale resultaten 69
longtumoren stadia therapie prognose Els De Droogh Pneumologie ZNA Middelheim
 longtumoren stadia therapie prognose smoking is cool!??? longtumoren > na WO II > roken en longtumoren 90 % mannen, 78% vrouwen aantal pakjaren > carcinogene stoffen in rook > asbest > radon, metalen,
longtumoren stadia therapie prognose smoking is cool!??? longtumoren > na WO II > roken en longtumoren 90 % mannen, 78% vrouwen aantal pakjaren > carcinogene stoffen in rook > asbest > radon, metalen,
Staging van het Bronchuscarcinoom
 1 Staging van het Bronchuscarcinoom Dr D Coeman Pneumoloog A.Z. St.-Dimpna, Geel Staging v/h bronchuscarcinoom 2 A/ NSCLC - TNM-classification B/ SCLC - VALSG (veterans s affairs lung study group) - TNM-classification
1 Staging van het Bronchuscarcinoom Dr D Coeman Pneumoloog A.Z. St.-Dimpna, Geel Staging v/h bronchuscarcinoom 2 A/ NSCLC - TNM-classification B/ SCLC - VALSG (veterans s affairs lung study group) - TNM-classification
CHIRURGIE BIJ LONGKANKER
 CHIRURGIE BIJ LONGKANKER Prof. Dr. P. De Leyn Kliniekhoofd Thoraxheelkunde Universitair Ziekenhuis Gasthuisberg Leuven Meeting Pneumologie Verpleegkundigen BVP/SVP meeting dec 2007 LEUVEN LUNG CANCER GROUP
CHIRURGIE BIJ LONGKANKER Prof. Dr. P. De Leyn Kliniekhoofd Thoraxheelkunde Universitair Ziekenhuis Gasthuisberg Leuven Meeting Pneumologie Verpleegkundigen BVP/SVP meeting dec 2007 LEUVEN LUNG CANCER GROUP
Video-Assisted Thoracic Surgery: Het einde van de thoracotomie?
 Brugge, 29-04-2017 Dr. Jan Lesaffer Borst- en thoracaal chirurg Dienst Algemene, Kinder- en Vaatheelkunde AZ Sint-Jan Brugge-Oostende, campus Brugge 1911 HC Jacobeus: diagnostische en therapeutische thoracoscopie
Brugge, 29-04-2017 Dr. Jan Lesaffer Borst- en thoracaal chirurg Dienst Algemene, Kinder- en Vaatheelkunde AZ Sint-Jan Brugge-Oostende, campus Brugge 1911 HC Jacobeus: diagnostische en therapeutische thoracoscopie
Slokdarmcarcinoom
 7.1.1. Slokdarmcarcinoom 1. Inleiding 1.1. Algemeen Kanker van de slokdarm betreft vnl. het plaveiselcelcarcinoom en het adenocarcinoom, in minder dan vijf procent is er sprake van andere histologie. Hoewel
7.1.1. Slokdarmcarcinoom 1. Inleiding 1.1. Algemeen Kanker van de slokdarm betreft vnl. het plaveiselcelcarcinoom en het adenocarcinoom, in minder dan vijf procent is er sprake van andere histologie. Hoewel
Bronchuscarcinoom Incidentiegegevens, initiële behandeling AZ Groeninge Kris Van Oortegem Pneumologie
 Bronchuscarcinoom 2002 Incidentiegegevens, initiële behandeling AZ Groeninge Kris Van Oortegem Pneumologie Bronchuscarcinoom 2002 (n=112) Kleincellig versus Niet-kleincellig kleincellig 18% niet-kleincellig
Bronchuscarcinoom 2002 Incidentiegegevens, initiële behandeling AZ Groeninge Kris Van Oortegem Pneumologie Bronchuscarcinoom 2002 (n=112) Kleincellig versus Niet-kleincellig kleincellig 18% niet-kleincellig
Stage. Clin staging. Treatment. Prognosis. Diagnosis. Evaluation. Early Node. Tumour. Loc advanced Metastasis. Advanced. Surgery
 Clin staging Stage Tumour Early Node Loc advanced Metastasis Advanced Treatment Surgery Diagnosis Evaluation pulmonary Chemotherapy Radiotherapy Combinations Prognosis cardiac general Univ Hospital Leuven
Clin staging Stage Tumour Early Node Loc advanced Metastasis Advanced Treatment Surgery Diagnosis Evaluation pulmonary Chemotherapy Radiotherapy Combinations Prognosis cardiac general Univ Hospital Leuven
Thoraxchirurgie. In Tergooiziekenhuizen
 Thoraxchirurgie In Tergooiziekenhuizen Waarvoor? Trauma Benigne afwijkingen Maligne afwijkingen Thorax trauma Benigne afwijkingen Pneumothorax Goedaardige tumoren Infekties Maligne afwijkingen Longcarcinoom
Thoraxchirurgie In Tergooiziekenhuizen Waarvoor? Trauma Benigne afwijkingen Maligne afwijkingen Thorax trauma Benigne afwijkingen Pneumothorax Goedaardige tumoren Infekties Maligne afwijkingen Longcarcinoom
CHIRURGIE BIJ LONGKANKER
 CHIRURGIE BIJ LONGKANKER Prof. Dr. P. De Leyn Diensthoofd Thoraxheelkunde Voorzitter competentiecentrum Heelkunde Universitair Ziekenhuis Gasthuisberg Leuven Postgraduaat Onderwijs Heelkunde Donderdag
CHIRURGIE BIJ LONGKANKER Prof. Dr. P. De Leyn Diensthoofd Thoraxheelkunde Voorzitter competentiecentrum Heelkunde Universitair Ziekenhuis Gasthuisberg Leuven Postgraduaat Onderwijs Heelkunde Donderdag
Dutch Lung Surgery Audit (DLSA)
") Dutch Lung Surgery Audit (DLSA) Beschrijving Dit overzicht toont de kwaliteitsindicatoren welke per 1 april 2014 ontsloten zullen worden in het kader van het getrapte transparantiemodel van DICA. De ontsluiting
Dutch Lung Surgery Audit (DLSA) Beschrijving Dit overzicht toont de kwaliteitsindicatoren welke per 1 april 2014 ontsloten zullen worden in het kader van het getrapte transparantiemodel van DICA. De ontsluiting
Lokaal-Gevorderd Niet-KleinCellig LongCarcinoma (LA-NSCLC)
") Lokaal-Gevorderd Niet-KleinCellig LongCarcinoma (LA-NSCLC) vrouw, 54j, 30 pakjaren toevallige vondst tumoraal letsel rechter longbk CT: letsel apicaal in rechterbk, tegenaan de pleura klierpakket rechts
Lokaal-Gevorderd Niet-KleinCellig LongCarcinoma (LA-NSCLC) vrouw, 54j, 30 pakjaren toevallige vondst tumoraal letsel rechter longbk CT: letsel apicaal in rechterbk, tegenaan de pleura klierpakket rechts
Casus oncologie,, D.R., 1930
 Casus oncologie,, D.R., 1930 Medische voorgeschiedenis 1992: prostatectomie wegens benigne prostaathypertrofie 2009: CVA met rechter hemiparese, volledige recuperatie 03/2013: paroxysmale VKF: echocor:
Casus oncologie,, D.R., 1930 Medische voorgeschiedenis 1992: prostatectomie wegens benigne prostaathypertrofie 2009: CVA met rechter hemiparese, volledige recuperatie 03/2013: paroxysmale VKF: echocor:
Behandelingsstrategie bij het Bronchuscarcinoma. Dr. Alida Vaes Pneumologie A.Z. St.-Dimpna Geel / H. Hartziekenhuis Mol
 1 Behandelingsstrategie bij het Bronchuscarcinoma Dr. Alida Vaes Pneumologie A.Z. St.-Dimpna Geel / H. Hartziekenhuis Mol 2 Type tumor APO Niet kleincellig longcarcinoom(nsclc) Kleincellig longcarcinoom
1 Behandelingsstrategie bij het Bronchuscarcinoma Dr. Alida Vaes Pneumologie A.Z. St.-Dimpna Geel / H. Hartziekenhuis Mol 2 Type tumor APO Niet kleincellig longcarcinoom(nsclc) Kleincellig longcarcinoom
Factsheet Indicatoren Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016
 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016") Factsheet en Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016 Inclusie en exclusie criteria DLCA-S Inclusie Alle chirurgische
Factsheet en Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016 Inclusie en exclusie criteria DLCA-S Inclusie Alle chirurgische
longcarcinoom: stadiëring en behandeling
 Hoe actueel is de CBO richtlijn? Niet-kleincellig longcarcinoom: stadiëring en behandeling Prof. dr. Harry J.M. Groen UMCG Groningen Wat moet er veranderen? TBNA? Plaats van EUS-FNA? Plaats van EBUS-FNA?
Hoe actueel is de CBO richtlijn? Niet-kleincellig longcarcinoom: stadiëring en behandeling Prof. dr. Harry J.M. Groen UMCG Groningen Wat moet er veranderen? TBNA? Plaats van EUS-FNA? Plaats van EBUS-FNA?
Factsheet Indicatoren Longcarcinoom (DLSA-DLRA) 2016
 2016") Factsheet en Longcarcinoom (DLSA-DLRA) 2016 Inclusie en exclusie criteria DLSA Inclusie Alle chirurgische thoracale (thoraxwand, pleurale, long en mediastinale) ingrepen, in te delen in: Resecties bij
Factsheet en Longcarcinoom (DLSA-DLRA) 2016 Inclusie en exclusie criteria DLSA Inclusie Alle chirurgische thoracale (thoraxwand, pleurale, long en mediastinale) ingrepen, in te delen in: Resecties bij
1. Inleiding: De nieuwe TNM classifikatie stadiering. - onvolledigheden / aanvullingen. 3. De N factor: hoe in kaart brengen.
 Mediastinum 1. Inleiding: De nieuwe TNM classifikatie stadiering 2. De N factor: impact op prognose: -vlgtnm - onvolledigheden / aanvullingen 3. De N factor: hoe in kaart brengen. 4. De N factor: impact
Mediastinum 1. Inleiding: De nieuwe TNM classifikatie stadiering 2. De N factor: impact op prognose: -vlgtnm - onvolledigheden / aanvullingen 3. De N factor: hoe in kaart brengen. 4. De N factor: impact
Echo-endoscopie. Dr. Mike Cool. AZ Damiaan Oostende UZ Leuven. Echo-endoscopie
 Echo-endoscopie Dr. Mike Cool AZ Damiaan Oostende UZ Leuven 1. Wat is echo-endoscopie? 2. Wat is de meerwaarde van echo-endoscopie? 3. Diagnostische toepassingen A. Oncologie 1. Slo kdarmcarcinoom 2. Maagcarcinoom
Echo-endoscopie Dr. Mike Cool AZ Damiaan Oostende UZ Leuven 1. Wat is echo-endoscopie? 2. Wat is de meerwaarde van echo-endoscopie? 3. Diagnostische toepassingen A. Oncologie 1. Slo kdarmcarcinoom 2. Maagcarcinoom
Maligne melanomen. Dr. N. Vancanneyt Prof. Dr. M. Stas Dienst Oncologische Heelkunde UZ Leuven
 Maligne melanomen Dr. N. Vancanneyt Prof. Dr. M. Stas Dienst Oncologische Heelkunde UZ Leuven Inhoud Introductie Diagnose & staging onderzoeken Classificatie Therapie Follow-up Introductie Maligne tumor
Maligne melanomen Dr. N. Vancanneyt Prof. Dr. M. Stas Dienst Oncologische Heelkunde UZ Leuven Inhoud Introductie Diagnose & staging onderzoeken Classificatie Therapie Follow-up Introductie Maligne tumor
Oesophaguscarcinoom Chirurgische Behandeling. Sylvia van der Horst, PA chirurgie Maart 2019
 Oesophaguscarcinoom Chirurgische Behandeling Sylvia van der Horst, PA chirurgie Maart 2019 Anatomie oesophagus/ maag Symptomen oesophaguscarcinoom Diagnostiek Behandeling oesophaguscarcinoom Postoperatieve
Oesophaguscarcinoom Chirurgische Behandeling Sylvia van der Horst, PA chirurgie Maart 2019 Anatomie oesophagus/ maag Symptomen oesophaguscarcinoom Diagnostiek Behandeling oesophaguscarcinoom Postoperatieve
Minimaal invasieve anatomische longresecties
 Minimaal invasieve anatomische longresecties Lieven Depypere, MD, PhD, FEBTS, FEBS/OG Thoraxheelkunde AZ Damiaan Thorax- en slokdarmheelkunde UZ Leuven lieven.depypere@uzleuven.be Minimaal invasieve anatomische
Minimaal invasieve anatomische longresecties Lieven Depypere, MD, PhD, FEBTS, FEBS/OG Thoraxheelkunde AZ Damiaan Thorax- en slokdarmheelkunde UZ Leuven lieven.depypere@uzleuven.be Minimaal invasieve anatomische
Slokdarmcarcinoom
 7.1.1. Slokdarmcarcinoom 1. Inleiding 1.1. Definitie Het cardiacarcinoom is een adenocarcinoom op de cardio-oesofageale overgang, waarbij de bulk van de tumor (in het resectiepreparaat) in de maag gelegen
7.1.1. Slokdarmcarcinoom 1. Inleiding 1.1. Definitie Het cardiacarcinoom is een adenocarcinoom op de cardio-oesofageale overgang, waarbij de bulk van de tumor (in het resectiepreparaat) in de maag gelegen
Gepersonaliseerde aanpak bij longkanker
 Gepersonaliseerde aanpak bij longkanker Dr. André VERSTRAETEN Dr. Elke GOVAERTS Dienst longziekten Pneumo-oncologie - Longkanker is de belangrijkste oorzaak van kankergerelateerde mortaliteit in beide
Gepersonaliseerde aanpak bij longkanker Dr. André VERSTRAETEN Dr. Elke GOVAERTS Dienst longziekten Pneumo-oncologie - Longkanker is de belangrijkste oorzaak van kankergerelateerde mortaliteit in beide
Factsheet Indicatoren Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016
 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016") Factsheet en Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016 Versie beheer: Datum Versie Mutatie Eigenaar 30-07-2016 2017.1 Aanpassingen
Factsheet en Longcarcinoom (DLCA) 2017 Start DLCA-S: 2012 (/2015 voor alle cardiothoracale centra) Start DLCA-R: 2013 Start DLCA-L: 2016 Versie beheer: Datum Versie Mutatie Eigenaar 30-07-2016 2017.1 Aanpassingen
Algemene opmerking: classificatie van toepassing op carcinomen met inbegrip van adenocarcinomen van de gastrooesofagale
 MAAG 1. Tumor: 1.1. TNM classificatie: Algemene opmerking: classificatie van toepassing op carcinomen met inbegrip van adenocarcinomen van de gastrooesofagale junctie. Tumor met epicentrum binnen 5 cm
MAAG 1. Tumor: 1.1. TNM classificatie: Algemene opmerking: classificatie van toepassing op carcinomen met inbegrip van adenocarcinomen van de gastrooesofagale junctie. Tumor met epicentrum binnen 5 cm
CHAPTER 8. Samenvatting
 CHAPTER 8 Samenvatting 108 Chapter 8 Samenvatting 109 Samenvatting Jaarlijks wordt wereldwijd bij 1,2 miljoen mensen de diagnose longkanker gesteld en overlijden 1,1 miljoen mensen aan deze ziekte. Hiermee
CHAPTER 8 Samenvatting 108 Chapter 8 Samenvatting 109 Samenvatting Jaarlijks wordt wereldwijd bij 1,2 miljoen mensen de diagnose longkanker gesteld en overlijden 1,1 miljoen mensen aan deze ziekte. Hiermee
Inhoud. 1. Epidemiologie 2. Pathologie 3. Klinische presentatie 4. Diagnostiek 5. TNM classificatie
 Slokdarmcarcinoom Inhoud 1. Epidemiologie 2. Pathologie 3. Klinische presentatie 4. Diagnostiek 5. TNM classificatie Epidemiologie: incidentie Globaal: Nummer 9 Hoge mortaliteit 1/20 kankersterfte Global
Slokdarmcarcinoom Inhoud 1. Epidemiologie 2. Pathologie 3. Klinische presentatie 4. Diagnostiek 5. TNM classificatie Epidemiologie: incidentie Globaal: Nummer 9 Hoge mortaliteit 1/20 kankersterfte Global
Beeldvorming bij gemetastaseerd mamma- en longcarcinoom Sebastiaan Franken, Fellow mammaradiologie Jeroen Bosch Ziekenhuis
 Beeldvorming bij gemetastaseerd mamma- en longcarcinoom Sebastiaan Franken, Fellow mammaradiologie Jeroen Bosch Ziekenhuis Casper van Everdingen, radioloog in het Diakonessenhuis Utrecht Disclosure belangen
Beeldvorming bij gemetastaseerd mamma- en longcarcinoom Sebastiaan Franken, Fellow mammaradiologie Jeroen Bosch Ziekenhuis Casper van Everdingen, radioloog in het Diakonessenhuis Utrecht Disclosure belangen
Tumoren van het anaal kanaal
 7.1.8. Tumoren van het anaal kanaal 1. Inleiding 1.1. Incidentie Aparte entiteit! Incidentie uitzonderlijk (2% van de digestieve tumoren) Incidentie 3v - 2m Gem. 65 jaar 2. Klinische presentatie De meeste
7.1.8. Tumoren van het anaal kanaal 1. Inleiding 1.1. Incidentie Aparte entiteit! Incidentie uitzonderlijk (2% van de digestieve tumoren) Incidentie 3v - 2m Gem. 65 jaar 2. Klinische presentatie De meeste
Bronchoscopie bij de diagnostiek en stadiëring van het bronchuscarcinoom : rol van nieuwe navigatietechnieken. Dr. Annelies Janssens Longarts
 Bronchoscopie bij de diagnostiek en stadiëring van het bronchuscarcinoom : rol van nieuwe navigatietechnieken Dr. Annelies Janssens Longarts Diagnose Stadiëring Duidelijke histologische diagnose Hoe uitgebreid
Bronchoscopie bij de diagnostiek en stadiëring van het bronchuscarcinoom : rol van nieuwe navigatietechnieken Dr. Annelies Janssens Longarts Diagnose Stadiëring Duidelijke histologische diagnose Hoe uitgebreid
Laarbeeklaan Brussel. Oncologisch Handboek. Richtlijnen Urologie. Testis
 Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen Urologie Testis V3.2014 Testis ICD-O C62 1 Inleiding De richtlijnen hebben betrekking tot kiemceltumoren van de testis, die meer dan 90% van
Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen Urologie Testis V3.2014 Testis ICD-O C62 1 Inleiding De richtlijnen hebben betrekking tot kiemceltumoren van de testis, die meer dan 90% van
Thoraxchirurgie Postgraduaat onderwijs 15/04/2016. M. De Waele, P. Lauwers, J. Hendriks, P. Van Schil Thorax- en Vaatheelkunde, UZA
 Thoraxchirurgie Postgraduaat onderwijs 15/04/2016 M. De Waele, P. Lauwers, J. Hendriks, P. Van Schil Thorax- en Vaatheelkunde, UZA OVERZICHT 1. Mediastinoscopie 2. Thoracoscopie 3. Thoracotomie 4. Complicaties
Thoraxchirurgie Postgraduaat onderwijs 15/04/2016 M. De Waele, P. Lauwers, J. Hendriks, P. Van Schil Thorax- en Vaatheelkunde, UZA OVERZICHT 1. Mediastinoscopie 2. Thoracoscopie 3. Thoracotomie 4. Complicaties
Slokdarm resectie. MDL onderwijs, M. de Maat, chirurg
 Slokdarm resectie MDL onderwijs, 11-03-2019 M. de Maat, chirurg Incidentie NL: 2850 patiënten per jaar ongeveer 50% operabel. Jaarlijks aantal nieuwe gevallen per 100.000 Nederlanders: 1990: ~5 2016: ~10
Slokdarm resectie MDL onderwijs, 11-03-2019 M. de Maat, chirurg Incidentie NL: 2850 patiënten per jaar ongeveer 50% operabel. Jaarlijks aantal nieuwe gevallen per 100.000 Nederlanders: 1990: ~5 2016: ~10
Leuvense Dagen voor Huisartsgeneeskunde 2012 PNEUMOLOGIE. Longkanker in de huisartspraktijk kristiaan.nackaerts@uzleuven.be
 Leuvense Dagen voor Huisartsgeneeskunde 2012 PNEUMOLOGIE Longkanker in de huisartspraktijk kristiaan.nackaerts@uzleuven.be Longkanker voor de huisartspraktijk Epidemiologie Etiologie Vroegtijdige detectie
Leuvense Dagen voor Huisartsgeneeskunde 2012 PNEUMOLOGIE Longkanker in de huisartspraktijk kristiaan.nackaerts@uzleuven.be Longkanker voor de huisartspraktijk Epidemiologie Etiologie Vroegtijdige detectie
Ontwikkelingen longkanker en maligne mesothelioom
 Ontwikkelingen longkanker en maligne mesothelioom Wat is de stand van zaken Frank Jacobs sept 2017 Disclosures Frank Jacobs (potentiële) belangenverstrengeling geen Voor bijeenkomst mogelijk relevante
Ontwikkelingen longkanker en maligne mesothelioom Wat is de stand van zaken Frank Jacobs sept 2017 Disclosures Frank Jacobs (potentiële) belangenverstrengeling geen Voor bijeenkomst mogelijk relevante
Casus Keuzes in de behandeling van slokdarmkanker
 Casus Keuzes in de behandeling van slokdarmkanker Prof. dr. Mark van Berge Henegouwen, chirurg Dr. W.J. Eshuis, chirurg L. Noteboom, verpleegkundig specialist Amsterdam UMC, locatie AMC 8 e Inhoud Presentatie
Casus Keuzes in de behandeling van slokdarmkanker Prof. dr. Mark van Berge Henegouwen, chirurg Dr. W.J. Eshuis, chirurg L. Noteboom, verpleegkundig specialist Amsterdam UMC, locatie AMC 8 e Inhoud Presentatie
Slokdarmresectie - Fit aan de Start. Feike Kingma Arts-onderzoeker Chirurgie, UMC Utrecht
 Slokdarmresectie - Fit aan de Start Feike Kingma Arts-onderzoeker Chirurgie, UMC Utrecht Slokdarmkanker Slokdarmkanker zit vrijwel altijd in de thoracale slokdarm Jaarlijks aantal nieuwe gevallen per 100.000
Slokdarmresectie - Fit aan de Start Feike Kingma Arts-onderzoeker Chirurgie, UMC Utrecht Slokdarmkanker Slokdarmkanker zit vrijwel altijd in de thoracale slokdarm Jaarlijks aantal nieuwe gevallen per 100.000
Het bronchuscarcinoma Incidentie, symptomen en diagnose. Dr. M. Delanote Pneumoloog A.Z. St.-Dimpna, Geel
 1 Het bronchuscarcinoma Incidentie, symptomen en diagnose Dr. M. Delanote Pneumoloog A.Z. St.-Dimpna, Geel 2 1. Incidentie 2. Etiologie 3. Types 4. Symptomen 5. Diagnose 1. Incidentie 3 Vlaamse liga tegen
1 Het bronchuscarcinoma Incidentie, symptomen en diagnose Dr. M. Delanote Pneumoloog A.Z. St.-Dimpna, Geel 2 1. Incidentie 2. Etiologie 3. Types 4. Symptomen 5. Diagnose 1. Incidentie 3 Vlaamse liga tegen
Reeks 13: Vergeten organen Avond
 Reeks 13: Vergeten organen Avond Zeldzame Thoracale Tumoren tumor voorste mediastinum / Thymoom Dr. Monique Hochstenbag Longarts MUMC kalfszwezerik No Disclosures Mediastinum Voorste mediastinum Thymus
Reeks 13: Vergeten organen Avond Zeldzame Thoracale Tumoren tumor voorste mediastinum / Thymoom Dr. Monique Hochstenbag Longarts MUMC kalfszwezerik No Disclosures Mediastinum Voorste mediastinum Thymus
Pancreascarcinoom en kansen voor de toekomst
 18 mei 2006 Jaarbeurs Utrecht Pancreascarcinoom en kansen voor de toekomst Jan Ouwerkerk Research Coördinator Oncologie Leids Universitair Medisch Centrum Pancreas Carcinoom Incidencie: 33.730 nieuwe patiënten
18 mei 2006 Jaarbeurs Utrecht Pancreascarcinoom en kansen voor de toekomst Jan Ouwerkerk Research Coördinator Oncologie Leids Universitair Medisch Centrum Pancreas Carcinoom Incidencie: 33.730 nieuwe patiënten
Behandeling van dikke
 Behandeling van dikke Item 1 Item 2 Item 3 darmkanker Annelies Holvoet Donderdag 24/05/2018 > DD/MM/JJJJ Titel van d Dikke darmkanker Ontstaan Behandeling Preventie Dikkedarmkanker in Vlaanderen Jaarlijks
Behandeling van dikke Item 1 Item 2 Item 3 darmkanker Annelies Holvoet Donderdag 24/05/2018 > DD/MM/JJJJ Titel van d Dikke darmkanker Ontstaan Behandeling Preventie Dikkedarmkanker in Vlaanderen Jaarlijks
Ontwikkelingen bij de chirurgie van het slokdarm- en maagcarcinoom
 Ontwikkelingen bij de chirurgie van het slokdarm- en maagcarcinoom Mark I. van Berge Henegouwen Chirurg, slokdarm en maagchirurgie Amsterdam UMC, locatie AMC GIOCA GE oncologisch congres, AMC 18 jan 2019
Ontwikkelingen bij de chirurgie van het slokdarm- en maagcarcinoom Mark I. van Berge Henegouwen Chirurg, slokdarm en maagchirurgie Amsterdam UMC, locatie AMC GIOCA GE oncologisch congres, AMC 18 jan 2019
Wetenschappelijke Vergadering Recente evoluties in de oncologische thoraxchirurgie
 Wetenschappelijke Vergadering Recente evoluties in de oncologische thoraxchirurgie Lieven Depypere, thoraxheelkunde, AZ Damiaan Oostende Consulent thoraxheelkunde UZ Gasthuisberg Leuven ldepypere@azdamiaan.be
Wetenschappelijke Vergadering Recente evoluties in de oncologische thoraxchirurgie Lieven Depypere, thoraxheelkunde, AZ Damiaan Oostende Consulent thoraxheelkunde UZ Gasthuisberg Leuven ldepypere@azdamiaan.be
Verplichte indicatoren die moeten worden aangeleverd aan Zorginstituut Nederland. Indicator nummer Indicatornaam
 Zorginstituut Nederland Kwaliteitsinstituut Eekholt 4 1112 XH Diemen Postbus 320 1110 AH Diemen www.zorginstituutnederland.nl T +31 (0)20 797 89 20 Transparantiekalender@zinl.nl Oplegger indicatorenset
Zorginstituut Nederland Kwaliteitsinstituut Eekholt 4 1112 XH Diemen Postbus 320 1110 AH Diemen www.zorginstituutnederland.nl T +31 (0)20 797 89 20 Transparantiekalender@zinl.nl Oplegger indicatorenset
Indicatorenrapportage Ziekenhuis: Rijnstate Ziekenhuis Jaar: 2018 Totaal aantal ingevoerde patiënten
 De inhoud van de basis- en indicatorenrapportages is onderhevig aan updates en aanpassingen. In dit logboek kunt u per registratie de wijzigingen in de rapportages terugvinden tot en met het vorige kalenderjaar.
De inhoud van de basis- en indicatorenrapportages is onderhevig aan updates en aanpassingen. In dit logboek kunt u per registratie de wijzigingen in de rapportages terugvinden tot en met het vorige kalenderjaar.
Lymfeknoop dissectie in borstcarcinoom, diagnostiek of therapie? Wim Demey, medische oncologie, Borstkliniek voorkempen
 Lymfeknoop dissectie in borstcarcinoom, diagnostiek of therapie? Wim Demey, medische oncologie, Borstkliniek voorkempen 85% via de axilla Mammaria interna alleen aantasting is zeldzaam
Lymfeknoop dissectie in borstcarcinoom, diagnostiek of therapie? Wim Demey, medische oncologie, Borstkliniek voorkempen 85% via de axilla Mammaria interna alleen aantasting is zeldzaam
TNM Classificatie Longcarcinoom
 Thomas Malfait Endoscopische Eenheid - Longziekten UZ Gent thomas.malfait@uzgent.be TNM Classificatie Longcarcinoom 4de Masterclass thoracale oncologie voor verpleegkundigen Dank aan Yannick Vande Weygaerde
Thomas Malfait Endoscopische Eenheid - Longziekten UZ Gent thomas.malfait@uzgent.be TNM Classificatie Longcarcinoom 4de Masterclass thoracale oncologie voor verpleegkundigen Dank aan Yannick Vande Weygaerde
Unilaterale diafragma hoogstand. MR Ghamati
 Unilaterale diafragma hoogstand. MR Ghamati Inleiding Etiologie Risicofactoren en oorzaken Diagnostisering Kliniek Diafragma plicatie Review Conclusie Etiologie Oorzaken van een hoogstand van hemidiafragma
Unilaterale diafragma hoogstand. MR Ghamati Inleiding Etiologie Risicofactoren en oorzaken Diagnostisering Kliniek Diafragma plicatie Review Conclusie Etiologie Oorzaken van een hoogstand van hemidiafragma
Richtlijn: Solitaire pulmonale nodule ( coin lesion )
") Richtlijn: Solitaire pulmonale nodule ( coin lesion ) Een solitaire pulmonale nodule (SPN) wordt radiologisch gedefinieerd als een intraparenchymateus longletsel met een diameter
Richtlijn: Solitaire pulmonale nodule ( coin lesion ) Een solitaire pulmonale nodule (SPN) wordt radiologisch gedefinieerd als een intraparenchymateus longletsel met een diameter
Oligometastasen: Echt of wishfull thinking? Dirk De Ruysscher, MD, PhD Radiation Oncologist University Hospitals Leuven/ KU Leuven Leuven, Belgium
 Oligometastasen: Echt of wishfull thinking? Dirk De Ruysscher, MD, PhD Radiation Oncologist University Hospitals Leuven/ KU Leuven Leuven, Belgium Casus 65-jaar oude blanke vrouw 20 pak jaren Gestopt met
Oligometastasen: Echt of wishfull thinking? Dirk De Ruysscher, MD, PhD Radiation Oncologist University Hospitals Leuven/ KU Leuven Leuven, Belgium Casus 65-jaar oude blanke vrouw 20 pak jaren Gestopt met
Niet-kleincellig Longkanker 2015. Sjaak Burgers s.burgers@nki.nl
 Niet-kleincellig Longkanker 2015 Sjaak Burgers s.burgers@nki.nl Adviesraadlid Adviseur AstraZeneca Boehringer Instituut AsbestSlachtoffers Patiëntenvereniging voor Asbestslachtoffers Te bespreken: Roken
Niet-kleincellig Longkanker 2015 Sjaak Burgers s.burgers@nki.nl Adviesraadlid Adviseur AstraZeneca Boehringer Instituut AsbestSlachtoffers Patiëntenvereniging voor Asbestslachtoffers Te bespreken: Roken
Robot geassisteerde slokdarm chirurgie. Dr. P.C. van der Sluis MD, PhD, Msc. AIOS Heelkunde jaar 6
 Robot geassisteerde slokdarm chirurgie Dr. P.C. van der Sluis MD, PhD, Msc. AIOS Heelkunde jaar 6 P.C.vandersluis-2@umcutrecht.nl Slokdarmkanker Jaarlijks: +/- 2000 nieuwe diagnoses Incidentie: 6% toename
Robot geassisteerde slokdarm chirurgie Dr. P.C. van der Sluis MD, PhD, Msc. AIOS Heelkunde jaar 6 P.C.vandersluis-2@umcutrecht.nl Slokdarmkanker Jaarlijks: +/- 2000 nieuwe diagnoses Incidentie: 6% toename
Dutch Lung Surgery Audit.Landelijke registratie van longresecties en overige thoracale chirurgie. DLSA
 Dutch Lung Surgery Audit.Landelijke registratie van longresecties en overige thoracale chirurgie. DLSA Vetgedrukte items zijn verplicht Versie: 2014-12-23 - v2.4.0 Patientgegevens Voor welk jaar gaat u
Dutch Lung Surgery Audit.Landelijke registratie van longresecties en overige thoracale chirurgie. DLSA Vetgedrukte items zijn verplicht Versie: 2014-12-23 - v2.4.0 Patientgegevens Voor welk jaar gaat u
Nederlandse introductie en samenvatting voor niet-ingewijden
 Nederlandse introductie en samenvatting voor niet-ingewijden 157 Introductie In de Westerse wereld is het aantal mensen dat slokdarmkanker krijgt de laatste jaren sterk toegenomen. In 1989 werd de diagnose
Nederlandse introductie en samenvatting voor niet-ingewijden 157 Introductie In de Westerse wereld is het aantal mensen dat slokdarmkanker krijgt de laatste jaren sterk toegenomen. In 1989 werd de diagnose
B. Hals (weke delen) Voor cervicale wervelkolom, zie rubrieken C en K. Inhoudsopgave 01 B 02 B 03 B 04 B 05 B 06 B 07 B 08 B 09 B 10 B 11 B 12 B 13 B
 Voor cervicale wervelkolom, zie rubrieken C en K. Inhoudsopgave 01 B 02 B 03 B 04 B 05 B 06 B 07 B 08 B 09 B 10 B 11 B 12 B 13 B") B. Hals (weke delen) Voor cervicale wervelkolom, zie rubrieken C en K Inhoudsopgave 1 B 2 B 3 B 4 B 5 B 6 B 7 B 8 B 9 B 1 B 11 B 12 B 13 B Palpabele schildkliernoduli en euthyreotische struma... 1 Lange
B. Hals (weke delen) Voor cervicale wervelkolom, zie rubrieken C en K Inhoudsopgave 1 B 2 B 3 B 4 B 5 B 6 B 7 B 8 B 9 B 1 B 11 B 12 B 13 B Palpabele schildkliernoduli en euthyreotische struma... 1 Lange
Richtlijn voor diagnostiek en behandeling van het plaveiselcelcarcinoom van de hypopharynx
 IX Richtlijn voor diagnostiek en behandeling van het plaveiselcelcarcinoom van de hypopharynx naar Algemeen 552 Epidemiologie 552 1. Screening 552 2. Diagnostiek 552 2.1 Anamnese 552 2.2 Fysische diagnostiek
IX Richtlijn voor diagnostiek en behandeling van het plaveiselcelcarcinoom van de hypopharynx naar Algemeen 552 Epidemiologie 552 1. Screening 552 2. Diagnostiek 552 2.1 Anamnese 552 2.2 Fysische diagnostiek
Laarbeeklaan Brussel. Oncologisch Handboek. Richtlijnen KNO. Larynx
 Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen KNO Larynx V2.2011 Larynxcarcinoom ICD-O C32.0, 1, 2, C10.1 Volgende regio s en subregio s worden beschreven: 1. Supraglottis (C32.1): Suprahyoidale
Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen KNO Larynx V2.2011 Larynxcarcinoom ICD-O C32.0, 1, 2, C10.1 Volgende regio s en subregio s worden beschreven: 1. Supraglottis (C32.1): Suprahyoidale
Pancreascarcinoom
 7.1.3. Pancreascarcinoom 1. Pancreasadenocarcinoma: diagnose en staging 1.1. Symptomen Zeer aspecifiek. 10% van de patiënten presenteren zich met nieuwe DM. Bij oudere patiënten is acute pancreatitis vaak
7.1.3. Pancreascarcinoom 1. Pancreasadenocarcinoma: diagnose en staging 1.1. Symptomen Zeer aspecifiek. 10% van de patiënten presenteren zich met nieuwe DM. Bij oudere patiënten is acute pancreatitis vaak
Laarbeeklaan Brussel. Oncologisch Handboek. Richtlijnen Urologie. Blaas
 Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen Urologie Blaas V3.2014 Blaas ICD-O C67 1 Inleiding De meerderheid van de patiënten (75-85%) vertoont oppervlakkige blaastumoren (stadium Tis,
Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen Urologie Blaas V3.2014 Blaas ICD-O C67 1 Inleiding De meerderheid van de patiënten (75-85%) vertoont oppervlakkige blaastumoren (stadium Tis,
Luchtwegen: luchtpijp. luchtwegen spirometrie. Longblaasjes: Alveolen longvolumes diffusie
 Interstitiële longziekten Prof. Dr. Guy Brusselle Dienst Longziekten UZ GENT BVP, 23/11/2013 Interstitiële longziekten (ILZ): Inleiding Kenmerken overzicht ILZ met gekende oorzaken ILZ met ongekende oorzaken:
Interstitiële longziekten Prof. Dr. Guy Brusselle Dienst Longziekten UZ GENT BVP, 23/11/2013 Interstitiële longziekten (ILZ): Inleiding Kenmerken overzicht ILZ met gekende oorzaken ILZ met ongekende oorzaken:
Nieuwe ontwikkelingen binnen de MDL-oncologie. Paul Fockens, MDL-arts AMC
 Nieuwe ontwikkelingen binnen de MDL-oncologie Paul Fockens, MDL-arts AMC Nieuwe ontwikkelingen MDL-oncologie De termen van 2012: Minimally invasive Patient centered Multi-modality Ageing population (Neo-)adjuvant
Nieuwe ontwikkelingen binnen de MDL-oncologie Paul Fockens, MDL-arts AMC Nieuwe ontwikkelingen MDL-oncologie De termen van 2012: Minimally invasive Patient centered Multi-modality Ageing population (Neo-)adjuvant
Peniscarcinoom. Regionale richtlijn IKMN, Versie: 1.1
 Peniscarcinoom Regionale richtlijn IKMN, Versie: 1.1 Laatst gewijzigd : 02-05-2003 Methodiek: Consensus based Verantwoording: Reg. WG urologische tumoren Inhoudsopgave Algemeen...1 Diagnostiek...2 Medisch
Peniscarcinoom Regionale richtlijn IKMN, Versie: 1.1 Laatst gewijzigd : 02-05-2003 Methodiek: Consensus based Verantwoording: Reg. WG urologische tumoren Inhoudsopgave Algemeen...1 Diagnostiek...2 Medisch
Indicatorenrapportage Ziekenhuis: Rijnstate Ziekenhuis Jaar: 2017 Totaal aantal ingevoerde patiënten
 The resource of this report item is not reachable. De inhoud van de basis- en indicatorenrapportages zijn onderhevig aan updates en aanpassingen. In dit logboek kunt u per registratie de wijzigingen in
The resource of this report item is not reachable. De inhoud van de basis- en indicatorenrapportages zijn onderhevig aan updates en aanpassingen. In dit logboek kunt u per registratie de wijzigingen in
Tx niet evalueerbaar T0 geen tumor
 COLON 1. Tumor: 1.1. TNM classificatie: T: primaire tumor Tx niet evalueerbaar T0 geen tumor Tis T1 carcinoma in situ: intra-epitheliaal of invasie lamina propria (niet doorheen muscularis mucosa) subclassificatie
COLON 1. Tumor: 1.1. TNM classificatie: T: primaire tumor Tx niet evalueerbaar T0 geen tumor Tis T1 carcinoma in situ: intra-epitheliaal of invasie lamina propria (niet doorheen muscularis mucosa) subclassificatie
Stadiering en triple diagnostiek van borst en oksel. Dr. P. Berteloot 10/2011
 Stadiering en triple diagnostiek van borst en oksel Dr. P. Berteloot 10/2011 Diagnostische beeldvorming Radiologisch onderzoek ter evaluatie van - klinische afwijking screenings gedetecteerde afwijking
Stadiering en triple diagnostiek van borst en oksel Dr. P. Berteloot 10/2011 Diagnostische beeldvorming Radiologisch onderzoek ter evaluatie van - klinische afwijking screenings gedetecteerde afwijking
Prof Dr D Van Raemdonck
 Interuniversitair Postgraduaat Onderwijs Heelkunde 4 de 5 de jaars ASO Heelkunde Vrijdag 8 maart 2013 Prof Dr D Van Raemdonck Dienst Thoraxheelkunde Universitaire Ziekenhuizen Leuven Definitie Thoracale
Interuniversitair Postgraduaat Onderwijs Heelkunde 4 de 5 de jaars ASO Heelkunde Vrijdag 8 maart 2013 Prof Dr D Van Raemdonck Dienst Thoraxheelkunde Universitaire Ziekenhuizen Leuven Definitie Thoracale
SLOKDARMKANKER. Bas Weusten, MDL-arts
 SLOKDARMKANKER Bas Weusten, MDL-arts b.l.a.weusten@umcutrecht.nl Slokdarmkanker Incidentie in NL Bij presentatie:
SLOKDARMKANKER Bas Weusten, MDL-arts b.l.a.weusten@umcutrecht.nl Slokdarmkanker Incidentie in NL Bij presentatie:
graad mitotische activiteit/10 hpf Ki67 index G1 <2 <2% G G3 >20 >20
 NEURO-ENDOCRIENE TUMOREN 1. Algemeen: Goed gedifferentieerde neuro-endocriene tumor: vroeger "carcinoïd". Goed gedifferentieerd carcinoma: "atypisch carcinoïd". Exclusief appendix. Opmerking: hooggradige
NEURO-ENDOCRIENE TUMOREN 1. Algemeen: Goed gedifferentieerde neuro-endocriene tumor: vroeger "carcinoïd". Goed gedifferentieerd carcinoma: "atypisch carcinoïd". Exclusief appendix. Opmerking: hooggradige
Mediastinale klierstagering van longkanker: nieuwe concepten Kurt G. Tournoy Thoracale Oncologie, Onze-Lieve-Vrouw Ziekenhuis Aalst; Universiteit Gent
 thoracale oncologie Peerreviewed article Mediastinale klierstagering van longkanker: nieuwe concepten Kurt G. Tournoy Thoracale Oncologie, OnzeLieveVrouw Ziekenhuis Aalst; Universiteit Gent Bij patiënten
thoracale oncologie Peerreviewed article Mediastinale klierstagering van longkanker: nieuwe concepten Kurt G. Tournoy Thoracale Oncologie, OnzeLieveVrouw Ziekenhuis Aalst; Universiteit Gent Bij patiënten
Heeft chirurgie of radiotherapie nog zin bij uitgezaaide prostaatkanker?
 Heeft chirurgie of radiotherapie nog zin bij uitgezaaide prostaatkanker? Wouter Everaerts Dienst urologie, Uzleuven @EveraertsW 16 september 2017 Natuurlijke evolutie van prostaatkanker PIN Gelokaliseerd
Heeft chirurgie of radiotherapie nog zin bij uitgezaaide prostaatkanker? Wouter Everaerts Dienst urologie, Uzleuven @EveraertsW 16 september 2017 Natuurlijke evolutie van prostaatkanker PIN Gelokaliseerd
Medische Publieksacademie 4 maart 2019
 4 maart 2019 YouTube 1 Ontwikkelingen in de longkankerzorg Dr. Ben Venmans, longarts Dr. Wouter van Geffen, longarts Frits Mostert, persvoorlichter MCL, moderator Programma 19.30 uur Dr. Ben Venmans: Longkanker:
4 maart 2019 YouTube 1 Ontwikkelingen in de longkankerzorg Dr. Ben Venmans, longarts Dr. Wouter van Geffen, longarts Frits Mostert, persvoorlichter MCL, moderator Programma 19.30 uur Dr. Ben Venmans: Longkanker:
Maligne pleura exsudaat
 Maligne pleura exsudaat Regionale richtlijn IKL, Versie: 1.1 Laatst gewijzigd : 25-10-2005 Methodiek: Consensus based Verantwoording: IKL werkgroep bronchuscarcinomen Inhoudsopgave Algemeen...1 Diagnostiek...2
Maligne pleura exsudaat Regionale richtlijn IKL, Versie: 1.1 Laatst gewijzigd : 25-10-2005 Methodiek: Consensus based Verantwoording: IKL werkgroep bronchuscarcinomen Inhoudsopgave Algemeen...1 Diagnostiek...2
Laarbeeklaan Brussel. Oncologisch Handboek. Richtlijnen KNO. Lip en mondholte
 Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen KNO Lip en mondholte V2.2011 Lip en mondholtecarcinoom ICD- O C00, C02-C06 Volgende regio s en subregio s worden beschreven: 1. De lip (C00):
Laarbeeklaan 101 1090 Brussel Oncologisch Handboek Richtlijnen KNO Lip en mondholte V2.2011 Lip en mondholtecarcinoom ICD- O C00, C02-C06 Volgende regio s en subregio s worden beschreven: 1. De lip (C00):
sequens is dan eerst chemotherapie, erna radiotherapie). Zo medisch inoperabel: o Radicale radiotherapie.
. Zo medisch inoperabel: o Radicale radiotherapie.") Richtlijn: Behandeling van vroege stadia NKCLC Deze richtlijn werd opgesteld in overeenkomst met de 7 de editie van het TNM systeem (TNM7), in voege vanaf begin 2010. Stadium IA (T1a-bN0) en Stadium IB
Richtlijn: Behandeling van vroege stadia NKCLC Deze richtlijn werd opgesteld in overeenkomst met de 7 de editie van het TNM systeem (TNM7), in voege vanaf begin 2010. Stadium IA (T1a-bN0) en Stadium IB
Longkanker; state of the art
 24 mei 2005 Jaarbeurs Utrecht Longkanker; state of the art Ivonne Schoenaker Verpleegkundig consulent oncologie Isala Klinieken / Zwolle Longkanker: The ugly facts Per jaar wordt bij 8000 nieuwe patiënten
24 mei 2005 Jaarbeurs Utrecht Longkanker; state of the art Ivonne Schoenaker Verpleegkundig consulent oncologie Isala Klinieken / Zwolle Longkanker: The ugly facts Per jaar wordt bij 8000 nieuwe patiënten
Hilaire pathologie. 4.1 Inleiding Radiologische kenmerken Oefencasus 12
 1 Hilaire pathologie.1 Inleiding 2.2 Radiologische kenmerken 2.2.1 Hilaire lymfeklierzwellingen 2.2.2 Endobronchiale afwijkingen.3 Oefencasus 12 2 Hoofdstuk Hilaire pathologie. 1 Inleiding De hilus is
1 Hilaire pathologie.1 Inleiding 2.2 Radiologische kenmerken 2.2.1 Hilaire lymfeklierzwellingen 2.2.2 Endobronchiale afwijkingen.3 Oefencasus 12 2 Hoofdstuk Hilaire pathologie. 1 Inleiding De hilus is
7.3.2. Baarmoedercarcinoom
 7.3.2. Baarmoedercarcinoom 1 Stadiëring 1.1 TNM-classificatie (7 th edition, 2009) Tx T0 Tis T1 T1a T1b T2 T3a T3b T4 Nx N0 N1 N2 M0 M1 Primaire tumor kan niet beoordeeld worden Geen evidentie voor primaire
7.3.2. Baarmoedercarcinoom 1 Stadiëring 1.1 TNM-classificatie (7 th edition, 2009) Tx T0 Tis T1 T1a T1b T2 T3a T3b T4 Nx N0 N1 N2 M0 M1 Primaire tumor kan niet beoordeeld worden Geen evidentie voor primaire
Chirurgische behandeling darmcarcinoom
 ONCOLOGISCH ZORGPROGRAMMA KEMPEN Regionale Vormingscel Oncologie Maandag 10 februari 2014 Dr. Maarten Michiels H.Hartziekenhuis Mol Chirurgische behandeling darmcarcinoom Fast facts Anatomie, fysiologie,
ONCOLOGISCH ZORGPROGRAMMA KEMPEN Regionale Vormingscel Oncologie Maandag 10 februari 2014 Dr. Maarten Michiels H.Hartziekenhuis Mol Chirurgische behandeling darmcarcinoom Fast facts Anatomie, fysiologie,
Image-guided stereotactic radiotherapy for early stage lung cancer: techniques and clinical outcomes. Samenvatting
 169 Image-guided stereotactic radiotherapy for early stage lung cancer: techniques and clinical outcomes Samenvatting Radiotherapie speelt een belangrijke rol in de curatieve behandeling van patiënten
169 Image-guided stereotactic radiotherapy for early stage lung cancer: techniques and clinical outcomes Samenvatting Radiotherapie speelt een belangrijke rol in de curatieve behandeling van patiënten
[(Verdenking op) longcarcinoom] [Mediastinumchirurgie] [Metastasectomie] [Overige ingreep]
![[(Verdenking op) longcarcinoom] [Mediastinumchirurgie] [Metastasectomie] [Overige ingreep]](/thumbs/30/14342614.jpg "[(Verdenking op) longcarcinoom] [Mediastinumchirurgie] [Metastasectomie] [Overige ingreep]") Dutch Lung Surgery Audit Vetgedrukte items zijn verplicht, grijs gedrukte items zijn optioneel Identificatie BSN-nummer Patiëntnummer in kliniek Geslacht... [Man] [Vrouw] Voorletters Tussenvoegsels Eigennaam
Dutch Lung Surgery Audit Vetgedrukte items zijn verplicht, grijs gedrukte items zijn optioneel Identificatie BSN-nummer Patiëntnummer in kliniek Geslacht... [Man] [Vrouw] Voorletters Tussenvoegsels Eigennaam
Pien de Haas en John de Klerk nucleair geneeskundigen Meander Medisch Centrum Amersfoort. 2e Mammacongres 28 januari 2011 Harderwijk
 Pien de Haas en John de Klerk nucleair geneeskundigen Meander Medisch Centrum Amersfoort 2e Mammacongres 28 januari 2011 Harderwijk Siemens Biograph true point PET/CT 40 slice Sinds 21 januari 2011 Sinds
Pien de Haas en John de Klerk nucleair geneeskundigen Meander Medisch Centrum Amersfoort 2e Mammacongres 28 januari 2011 Harderwijk Siemens Biograph true point PET/CT 40 slice Sinds 21 januari 2011 Sinds
Immuuntherapie: resultaten tot nu toe bij patiënten met een longcarcinoom Willemijn Theelen
 Immuuntherapie: resultaten tot nu toe bij patiënten met een longcarcinoom 15-06-2017 Willemijn Theelen w.theelen@nki.nl Risicofactoren Longcarcinoom Roken in 90% de oorzaak Passief roken : 1,2-1,3 x verhoogd
Immuuntherapie: resultaten tot nu toe bij patiënten met een longcarcinoom 15-06-2017 Willemijn Theelen w.theelen@nki.nl Risicofactoren Longcarcinoom Roken in 90% de oorzaak Passief roken : 1,2-1,3 x verhoogd
Multidisciplinaire behandeling van patient met een renaalcelcarcinoom
 Multidisciplinaire behandeling van patient met een renaalcelcarcinoom Introductie via een case-report Dr. Karen Heyrman, huisarts Initiële symptomen? Klassieke triade: (10%) Hematurie Flankpijn Palpabele
Multidisciplinaire behandeling van patient met een renaalcelcarcinoom Introductie via een case-report Dr. Karen Heyrman, huisarts Initiële symptomen? Klassieke triade: (10%) Hematurie Flankpijn Palpabele
Henderyckx Annemie hoofdverpleegkundige dienst longziekten campus Brugge. verpleegkundig Oncologisch congres AZ Sint Jan AV 16/03/2013
 Laat hem zijn sigaretje maar roken, zeggen zijn vrienden rond de toog als hij even naar buiten verdwijnt. Nu hij longkanker heeft, maakt het toch niet meer uit. verpleegkundig Oncologisch congres AZ Sint
Laat hem zijn sigaretje maar roken, zeggen zijn vrienden rond de toog als hij even naar buiten verdwijnt. Nu hij longkanker heeft, maakt het toch niet meer uit. verpleegkundig Oncologisch congres AZ Sint
Incidentie op topografie
 Kankerregistratie AZ Groeninge incidentiejaar 2004 Incidentie op topografie Incidentiejaar 2004 Incidentiejaar 2003 Incidentiejaar 2002 ORL: 62 54 Gastro-intestinaal: 270 245 Oesofagus 24 11 Maag 34 21
Kankerregistratie AZ Groeninge incidentiejaar 2004 Incidentie op topografie Incidentiejaar 2004 Incidentiejaar 2003 Incidentiejaar 2002 ORL: 62 54 Gastro-intestinaal: 270 245 Oesofagus 24 11 Maag 34 21
TP Indicatorenrapportage 2016 Ziekenhuis: Rijnstate Ziekenhuis Jaar: 2016
 De nummering van de indicatoren is gebaseerd op de documenten te vinden op: DICA/Transparantieportaal TP Indicatorenrapportage 2016 Ziekenhuis: Rijnstate Ziekenhuis Jaar: 2016 Structuurindicatoren 1. patiënten
De nummering van de indicatoren is gebaseerd op de documenten te vinden op: DICA/Transparantieportaal TP Indicatorenrapportage 2016 Ziekenhuis: Rijnstate Ziekenhuis Jaar: 2016 Structuurindicatoren 1. patiënten
Casus: Lokaal gevorderd Pancreascarcinoom (LAPC) Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG
 Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG") Casus: Lokaal gevorderd Pancreascarcinoom (LAPC) Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG no disclosures Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG Pancreascarcinoom Slechte
Casus: Lokaal gevorderd Pancreascarcinoom (LAPC) Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG no disclosures Olivier Busch HPB Chirurg, AMC Amsterdam Voorzitter DPCG Pancreascarcinoom Slechte
Larynxcarcinoma 10/03/2013. Heesheid en vroegdiagnostiek bij middel van narrow band imaging (NBI) en orgaansparende heelkunde bij larynxcarcinoma
 en orgaansparende heelkunde bij larynxcarcinoma") 1 Heesheid en vroegdiagnostiek bij middel van narrow band imaging (NBI) en orgaansparende heelkunde bij larynxcarcinoma Prof. Dr. Olivier Vanderveken Dienst NKO, Hoofd en Halsheelkunde UZA Faculteit Geneeskunde
1 Heesheid en vroegdiagnostiek bij middel van narrow band imaging (NBI) en orgaansparende heelkunde bij larynxcarcinoma Prof. Dr. Olivier Vanderveken Dienst NKO, Hoofd en Halsheelkunde UZA Faculteit Geneeskunde
Richtlijn voor diagnostiek en behandeling van het carcinoom van de neusholte, neusbijholten en het vestibulum nasi
 XII Richtlijn voor diagnostiek en behandeling van het carcinoom van de neusholte, neusbijholten en het vestibulum nasi naar Algemeen 568 Epidemiologie 568 1. Screening 568 2. Diagnostiek 568 2.1 Anamnese
XII Richtlijn voor diagnostiek en behandeling van het carcinoom van de neusholte, neusbijholten en het vestibulum nasi naar Algemeen 568 Epidemiologie 568 1. Screening 568 2. Diagnostiek 568 2.1 Anamnese
BASISPRINCIPES VAN KANKER
 BASISPRINCIPES VAN KANKER Prof.dr. D.J. Ruiter Afdeling Pathologie Cursus Introductie in de Fundamentele en Klinische Oncologie HET BEGRIP KANKER? a.alle gezwelgroei b.alle kwaadaardige gezwelgroei c.alle
BASISPRINCIPES VAN KANKER Prof.dr. D.J. Ruiter Afdeling Pathologie Cursus Introductie in de Fundamentele en Klinische Oncologie HET BEGRIP KANKER? a.alle gezwelgroei b.alle kwaadaardige gezwelgroei c.alle
FDG-PET in de respiratoire oncologie. Prof. Dr. Christophe Deroose Dienst Nucleaire Geneeskunde
 FDG-PET in de respiratoire oncologie Prof. Dr. Christophe Doose Dienst Nucleaire Geneeskunde Casus 1 Man, 65 jaar oud Medische voorgeschiedenis: Atiële hptensie Pcutane dilatatie a. femoralis supficialis
FDG-PET in de respiratoire oncologie Prof. Dr. Christophe Doose Dienst Nucleaire Geneeskunde Casus 1 Man, 65 jaar oud Medische voorgeschiedenis: Atiële hptensie Pcutane dilatatie a. femoralis supficialis
Prof Dr Dirk Van Raemdonck
 Interuniversitair Postgraduaat Onderwijs Heelkunde 4 de 5 de jaars ASO Heelkunde Woensdag 10 Oktober 2018 Prof Dr Dirk Van Raemdonck Dienst Thoraxheelkunde Universitaire Ziekenhuizen Leuven Definitie Thoracale
Interuniversitair Postgraduaat Onderwijs Heelkunde 4 de 5 de jaars ASO Heelkunde Woensdag 10 Oktober 2018 Prof Dr Dirk Van Raemdonck Dienst Thoraxheelkunde Universitaire Ziekenhuizen Leuven Definitie Thoracale
Zeldzame Thoracale Tumoren tumor voorste mediastinum
 Zeldzame Thoracale Tumoren tumor voorste mediastinum Monique Hochstenbag OncoZon Januari 2018 No Disclosures Proces voorste mediastinum Man 41-jaar Drukkend gevoel op de borst, moeheid, verminderde inspanningstolerantie
Zeldzame Thoracale Tumoren tumor voorste mediastinum Monique Hochstenbag OncoZon Januari 2018 No Disclosures Proces voorste mediastinum Man 41-jaar Drukkend gevoel op de borst, moeheid, verminderde inspanningstolerantie
KWALITEITSINDICATOREN VOOR ONCOLOGIE: BORSTKANKER Fase 1: validatie van de individuele resultaten Ziekenhuis 86
 1 KWALITEITSINDICATOREN VOOR ONCOLOGIE: BORSTKANKER Fase 1: validatie van de individuele resultaten Ziekenhuis 86 2 1. BESCHRIJVENDE STATISTIEK Tabel 1: Invasieve borstkanker en ductaal carcinoma in situ
1 KWALITEITSINDICATOREN VOOR ONCOLOGIE: BORSTKANKER Fase 1: validatie van de individuele resultaten Ziekenhuis 86 2 1. BESCHRIJVENDE STATISTIEK Tabel 1: Invasieve borstkanker en ductaal carcinoma in situ