Late effects of cancer treatment
|
|
|
- Augusta Vermeiren
- 8 jaren geleden
- Aantal bezoeken:
Transcriptie
1 19 mei 2009 Jaarbeurs Utrecht Late effects of cancer treatment Toepassen van evidence! Annelies Manenschijn MANP i.o. Isala klinieken Zwolle

2 Inhoud Aanleiding Cardiovasculaire gevolgen Pulmonale gevolgen Secundaire maligniteiten Overige late effecten Care plan USA Nacontrole in de oncologie

3 Aanleiding Toename survivors, 60% overleving na 5 jaar Toename als gevolg van meer complexe behandelingen Rapport: From Cancer Patient to Cancer Survivor: Lost in Transition. 1 Rapport: Nacontrole in de oncologie. 2 1 Hewitt, M., Greenfield, S., & Stovall, E. (2006) 2 Gezondheidsraad (2007)

4

5 Chemotherapie: cardio-vasculaire aandoeningen Anthracyclines: Ventriculaire dysfunctie Cardiomyopathie Hartfalen Alkylerende middelen (platinum, cyclofosfamide): Endotheliale schade Atherosclerose Metabool syndroom Carver J, et al (2007)

6

7 Risicofactoren anthracycline cardiomyopathie Patiëntenkenmerken: < 18 jaar bij start behandeling > 65 jaar bij start behandeling Bestaande hypertensie, reeds bestaande cardiale afwijking Zwangerschap Intensief sporten Carver J, et al (2007)

8 Risicofactoren anthracycline cardiomyopathie Kenmerken behandeling: Cumulatieve dosering 300 mg/m 2 doxorubicine of 600 mg/m 2 epirubicine Radiotherapie op het mediastinum Combinatie chemotherapie Langere tijd na behandeling Carver J, et al (2007)

9 Anthracyclines: Probability of Developing HF

10 Radiotherapie: Cardiovasculair Incidentie cardiale afwijkingen Piek 4-6 jr na behandeling 10 tot 30% 5 tot 10 jr na behandeling Tot 88% asymptomatische afwijkingen Studie: Hodgkin post-mediastinaal RT 2.2 tot 7.2 RR voor fatale cardiovasculaire ziekte Manifestatie 5 10 jr na behandeling 25% van de gerelateerde sterfte Carver J, et al (2007)

11 Radiotherapie: Mediastinum, thorax, mantelveld: Gevaarlijk voor álle hartstructuren Mogelijk tot jaren na radiotherapie Risicofactoren: Leeftijd < 18 jaar Dosis > Gy Combinatie met anthracyclines Verbeteren technieken RT doet incidentie dalen.

12 Interventie Preventie: Voorlichting Risicofactoren (overgewicht, beweging etc.) Tijdige behandeling: β-blokker, ACE-remmer, diuretica, etc. (niet bewezen!) High-risk groepen: elke 5 jr ECG Verwijzing cardioloog Carver J, et al (2007)

13 Pulmonale aandoeningen Verminderde longfunctie Pneumonieën (Bleomycine en/of radiotherapie) Fibrose Stamceltransplantaties: Bronchiolitis obliterans Idiopatische pneumonie Interstitiële pneumonie Kattlove & Winn (2003) Carver J, et al (2007) Gospodarowicz M. (2008)
 Carver J, et al (2007)")
14 Pulmonale aandoeningen: risicofactoren Behandelingsgerelateerd: Radiotherapie: Dosis (> 10 Gy) Volume Longkanker Chemotherapie: Bleomycine Lomustine Carmustine SCT Overige factoren: Leeftijd Roken nierfunctie Zuurstofopname Afbouwen steroïden Carver J, et al (2007) Friedman & Constine (2006)
")
15 Pulmonale aandoeningen Screening: Anamnese Op geleide van klachten verder onderzoek: Peakflow meten Saturatie Interventies: Voorlichting: Roken Griepvaccinatie Steroïdengebruik Verwijzing longarts

16 Secundaire maligniteiten 14% hogere kans op een nieuwe maligniteit Oorzaken: Genetisch Leefstijl Behandeling gerelateerd Curtis RE, et al (2006) Travis, Lois B. (2006)
")
17 Secundaire maligniteiten Chemotherapie: Alkylerende middelen t-mds/aml en blaasca Topo-isomeraseremmers t-mds/aml Platina: langdurig in lichaam aanwezig! t-mds/aml Tamoxifen: Endometriumca Sarcoom uterus

18 Secundaire maligniteiten Radiotherapie: M Hodgkin mammaca Schildklierregio schildklierca Craniale RT hersentumoren Stamceltransplantatie: Autoloog t-mds/aml Allogeen solide tumor

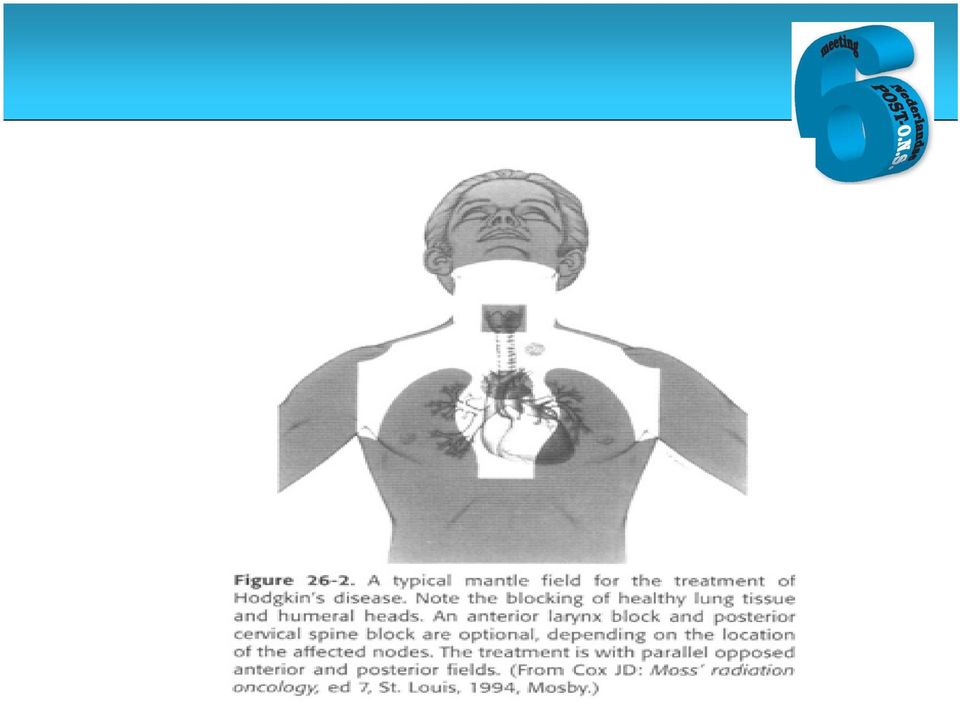
19 Mantle radiotherapy
20 Secundaire maligniteiten Incidentie per ziektebeeld: Mammaca 4% bij tamoxifengebruik Prostaatca tegenstrijdige cijfers Hodgkin 1,5 10% NHL 5% Hoofd-/halsca geen indicatie secundaire maligniteit

21 Overige late effecten Hypothyreoïdie Osteoporose Neuropathieën Cognitief Vruchtbaarheidsproblematiek Psychisch Nierfalen Groeistoornissen
22 Cancer Treatment Summary and Care Plan Institute of Medicine Report: From Cancer Patient to Cancer Survivor: Lost in Transition Recommendation #2: Patients completing primary treatment should be provided with a comprehensive care summary and follow up plan that is clearly and effectively explained. This Survivorship Care Plan should be written by the principal provider(s) who coordinated oncology treatment. This service should be reimbursed by thirdparty payors of health care. Oncology nurses could play a key role. Hewitt, M., Greenfield, S., & Stovall, E. (2006)
23 Casus Mw. LJ 36 jr invasief ductaal mammaca links (T1N1M0) Tumor = 1.5 cm; 2/10 LNN + ER positief, PR negatief, HER-2 negatief Lumpectomie + SN, later OKD RT linker borst 4 x AC, gevolgd door 4 x paclitaxel Exemestane + Triptorelin
24
25
26 OncoLink OncoLife Survivorship Care Plan Lance Armstrong Foundation and OncoLink care plan Binnenkort op
27
28 Survivorship care plan All survivors: Coordinating Your Care Risk of a second cancer Fatigue Risks Related to Medications Risk of Developing Bladder Cancer Risk of Bladder or Urinary Tract Toxicities Risk of Developing Osteoporosis Risk for Cardiac (Heart) Problems Related to Anthracycline Chemotherapies Fertility Concerns for Female Survivors Peripheral Neuropathy Sexuality Concerns for Female Survivors Side Effects while taking Aromatase Inhibitors Skin Toxicities Understanding "Chemo-brain Surgery Side Effects Lumpectomy Lymph Node Removal (Dissection) Sentinel Node Biopsy Radiation Side Effects Heart / Cardiovascular Lung Bone Skin Lymph nodes Radiation for breast cancer (after lumpectomy)
29
30 Nacontrole in de oncologie Doelen onderscheiden, inhoud onderbouwen. Nazorg richten op: 1. Voorlichten, signaleren, begeleiden en behandelen van gevolgen van therapie 2. Vroege detectie recidieven, metastasen en nieuwe tumoren 3. Evaluatie medisch handelen Programmatisch aangeboden Per tumorvorm verschillend Gezondheidsraad (2007)
31 Resultaat binnen 5 jaar a. Elke patiënt krijgt na de behandeling een nazorgplan met info over: Lichamelijke en psychosociale gevolgen van ziekte en behandeling Wenselijkheid en inrichting van nacontrole Bij afsluiting instructie en afspraken over blijvende aandachtspunten b. Voor alle tumortypen zijn programma s van nacontrole opgezet volgens geadviseerde systematiek Gezondheidsraad (2007)
32 CBO-richtlijn mammacarcinoom (2008)
33 Bronnen Carver J, Shapiro C, Ng A, Jacobs L, Schwartz C, Virgo K, Hagerty K, Somerfield M, Vaughn D. (2007). American Society of Clinical Oncology Clinical Evidence Review on the Ongoing Care of Adult Cancer Survivors: Cardiac and Pulmonary Late Effects. Journal of Clinical Oncology, ASCO Special Article, 25, 25: Curtis RE, Freedman DM, Ron E, Ries LAG, Hacker DG, Edwards BK, Tucker MA, Fraumeni JF Jr. (eds.). New Malignancies Among Cancer Survivors: SEER Cancer Registries, National Cancer Institute. NIH Publ. No Bethesda, MD, Friedman & Constine (2006). Late effects of treatment for Hodgkin s Lymphoma. JNCCN 4(3), Gezondheidsraad. Nacontrole in de oncologie. Doelen onderscheiden, inhoud onderbouwen. Den Haag: Gezondheidsraad, 2007; publicatienummer 2007/10. Gospodarowicz M. (2008). Hematol Oncol Clin North Am.(2): Hewitt M, Greenfield S, Stovall E. (2006). From Cancer Patient to Cancer Survivor: Lost in Transition. Washington, D.C.: The National Academies Press. Kattlove & Winn (2003). CA: Ca Jnl Clinicians 53(3), Travis, Lois B. (2006) The Epidemiology of Second Primary Cancers. Cancer Epidemiol Biomarkers Prev. 15 (11),